Bariatric surgery proves safe and effective for obese adolescents
Metabolic and bariatric surgery is emerging as a valuable therapeutic option for adolescents with severe obesity, offering weight loss and the reversal of cardiometabolic diseases.
Bariatric surgery proves safe and effective for obese adolescents
Metabolic and bariatric surgery (MBS) is emerging as a valuable therapeutic option for adolescents with severe obesity, offering substantial weight loss and the reversal of cardiometabolic diseases. While initial interventions for youth typically focus on lifestyle modifications, such programs often lack the durability to mitigate medical complications in those with extreme disease profiles.
Adolescents with severe obesity face higher risks of impaired quality of life and shorter life expectancy compared to peers with normal weight. Comorbidities such as hypertension, dyslipidemia, obstructive sleep apnea, and type 2 diabetes are commonplace in this group. According to research, type 2 diabetes in young people can take a more aggressive form, leading to earlier needs for pharmacological escalation and frequent end-stage complications in early adulthood.
Surgical Options and Clinical Guidelines
Current medical standards for adolescent MBS largely mirror adult guidelines. The 2018 American Society for Metabolic and Bariatric Surgery (ASMBS) guidelines recommend considering surgery for adolescents with a body mass index (BMI) ≥140% of the 95th percentile, or ≥120% of the 95th percentile if an associated comorbidity exists. These comorbidities include fatty liver disease, insulin resistance, hyperlipidemia, hypertension, type 2 diabetes, or obstructive sleep apnea.
The guidelines do not set a fixed age or pubertal stage for qualification. Instead, candidates are evaluated on a case-by-case basis, though patients must show the motivation to comply with treatment regimens. While substance abuse or untreated psychiatric challenges may delay surgery, they are not usually fixed contraindications. A 2022 update endorsed by the International Federation for Surgery for Obesity and ASMBS further notes that history of trauma, autism spectrum disorder, and developmental delay are increasingly not viewed as contraindications.
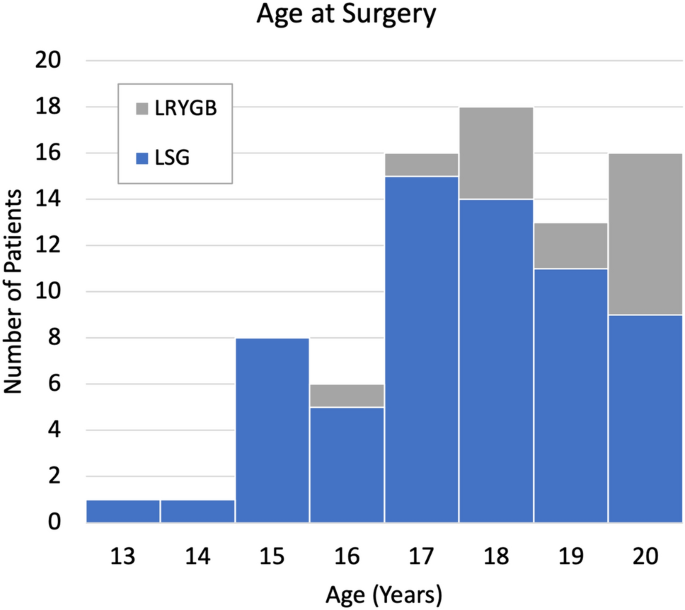
Two primary procedures are currently in common use:
- Laparoscopic sleeve gastrectomy (SG): The most performed procedure in adolescents today, this irreversible surgery removes more than 75% of the stomach to create a tube-shaped remnant.
- Laparoscopic Roux-en-Y gastric bypass (RYGB): Once the predominant method prior to 2010, this reversible procedure reorganizes the gastrointestinal tract to bypass most of the stomach and duodenum.
Adjustable gastric bands were previously used but have declined in popularity due to the frequent need for revisional surgery.
Weight Loss and Health Outcomes
Data indicates that weight loss and safety profiles in adolescents are similar to those seen in adults. In the Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS) study, participants who underwent SG lost a mean 27% of total body weight (TBW) over the first 3 years, representing a BMI reduction of 13 kg/m2. Similarly, Teen-LABS participants who had RYGB saw a 26% TBW loss after 5 years.
Other studies report varying long-term success. The Adolescent Morbid Obesity Surgery (AMOS) study observed a 28% TBW loss five years after RYGB. The Follow-up of Adolescent Bariatric Surgery at 5+ years (FABS5+) study reported a 29% TBW reduction and a BMI reduction of 16.9 kg/m2 after a mean of 8 years. A separate cohort of 96 young people with a median age of 19 showed a mean TBW reduction of 31.3%.
The benefits extend beyond weight. In the adolescent RYGB cohort of the Teen-LABS study, the overall prevalence of diabetes was reduced at 5 years, with no participants requiring antidiabetic medication at follow-up. Other studies showed a 58% to 100% remission of elevated blood pressure following MBS. The AMOS study also noted improvements in walking distance and maximal oxygen consumption at 1 and 2 years after gastric bypass.
Risks and Psychosocial Considerations
Surgery is not without risks. There is a potential for long-term nutritional deficiencies, particularly after RYGB, necessitating lifelong supplementation of iron, calcium, vitamin D, and vitamin B12. Bone mineral density may decrease across the first 2 years after surgery, though it typically remains within the normal range. Additionally, sleeve gastrectomy carries a substantial risk of developing reflux due to the high-pressure nature of the remnant stomach.
Psychological support is critical, as adolescents with severe obesity often report higher levels of depression and anxiety. While early postoperative data suggested mood improvements, long-term data from the AMOS study indicates these changes are often transient, with mean levels returning toward baseline after 2 years. However, sustained improvements in eating-related problems—such as binge eating and emotional eating—have been observed 4 and 5 years after surgery.
Multidisciplinary Integration
Effective care requires a specialist tertiary center with a multidisciplinary team, including pediatric psychologists or psychiatrists and infrastructure designed for high-BMI patients, such as floor-mounted toilets and larger beds. The need for coherent clinical guidelines and routine long-term follow-up remains a priority for the medical community.


